Most clinicians agree that hospitalisation can save a life, but it doesn’t fix the problem. That work takes place outside the hospital, and it’s a slow process, writes mental health nurse Duncan Milne.
Content warning: This piece discusses disordered eating and its treatment. Please take care.
The recent publicity around the tragic death of a young person suffering from an eating disorder, and family members’ criticism of the care agencies involved, has highlighted the challenges of treating people with disordered eating.
Anorexia nervosa (AN) is both hard to treat and very life threatening – it’s often described as the most lethal of the mental health conditions. People with AN typically devote much of their life to managing their weight and food intake, and the disorder can lead people to extremes as they try to achieve their weight goals – lying, cheating, hiding food and drinking water to mask weight loss are all common. Arguments are common, and can be heated. People with AN usually do not see their own bodies as others do, and may be unable to see why others are so worried about them. Research has shown that people with AN significantly overstate the size of their body, for example when asked to draw a life-sized outline, which may end up much larger than the reality. This distorted view can make it very hard to reason with people with AN, as they genuinely may not see what you see.
Treatment in the community takes a therapeutic approach, helping the person to look at their eating, understand what purpose this food restriction serves in their life, and figure out how to live a life in a healthy-sized body. Therapists often work with the whole family, examining attitudes toward food and supporting everyone to make change. It can take years, and people often need repeated periods of treatment through their lives as challenges come and go.
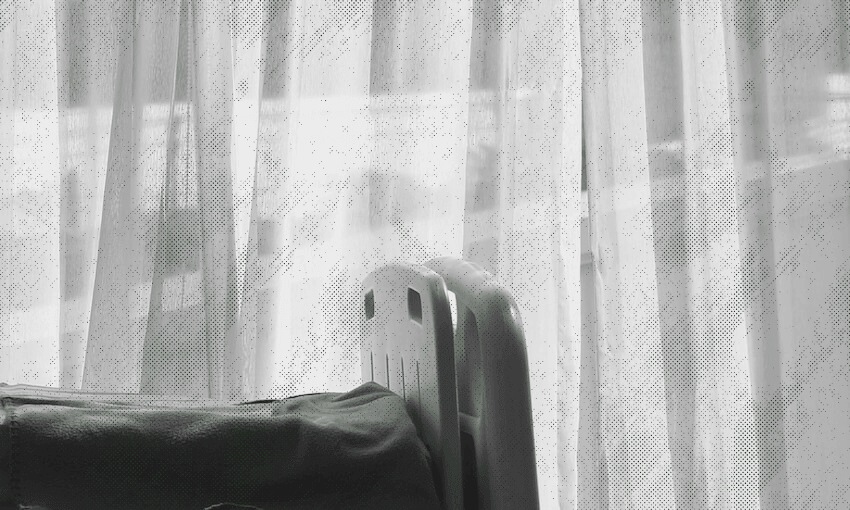
But if you’re too skinny, or if your blood results are too alarming, everything changes. Hospitalisation can be necessary when people are very underweight and at risk of medical consequences such as heart attack. If you live in the right city, this might happen in one of the scarce specialist mental health facilities for young people, but more likely the person will be in a hospital ward, surrounded by sick adults and cared for by staff who are well-meaning but may not have much clinical experience of AN.
Inpatient treatment is focused on eating and weight, so it is very confronting for a person who doesn’t think they need help. Refeeding is a process of close supervision during and after meals, careful oversight of physical activity, and close medical attention. Over-feeding can be lethal, so frequent weighing and blood tests are essential. Sometimes, supervision even in the toilet is necessary. Overnight checks are frequent, both to check they’re OK but also to ensure they’re not covertly exercising or pushing their blankets off (cold induces shivers, which burns calories).
Hospitalisation is brutal. It is intrusive and overwhelming. You are supervised in the most intimate moments, and it feels like there is no respite from eating, weighing or talking about food. Your whole day is confronting and upsetting. You are constantly being measured and prodded. You feel judged and criticised. Hospital staff may be unsympathetic, or feel like you are “taking up a bed”. Nobody trusts you, everybody tells you what to do and where to be, what to eat, and even how to sit.
People might agree to go into hospital the first time, but rarely the second. This can mean that the Mental Health Act (MHA) is used. The MHA provides for treatment against a person’s will, as long as two conditions are met. The first is that there must be a mental disorder, and the second is that there must be significant risk of harm to the person or another. Both conditions can be met in a person with AN, noting that the risk is to themselves – significant risk to others is not common.
However, compelling treatment can be traumatising, dehumanising and distressing, especially when you strongly disagree with the need for treatment in the first place. This means that, while the MHA is often literally lifesaving in a crisis, it can be counter-productive in the longer term. All parents know that forcing your child to do something might solve the problem you have now, but it probably won’t solve that problem tomorrow. And if the long-term solution is learning to have a healthy relationship with food, it’s no surprise if forcing food on someone does not move them closer to this goal.
Little wonder, then, that many people with AN describe hospitalisation as the worst experience of their lives. Sometimes it feels like people change their eating behaviours because they are so scared of going back to hospital. It might be effective, but it’s not something to be proud of. So most clinicians agree that hospitalisation can save a life, but it doesn’t fix the problem. That work takes place outside the hospital, and it’s slow work. And given people with AN may not agree that they even have a problem, treatment is gentle and kind, with a focus on building a trusting therapeutic relationship. When a person always has the choice to walk out or just stop participating, the relationship is vital and everything is negotiable – so force or compulsion has no place in this therapy, only calmness and respect. There are no shortcuts. It can also be scary, because people are out in the world making their own decisions, and they may not always be good ones.