
The practice of seclusion has been controversially used in mental healthcare in Aotearoa for years. Three health workers share what’s been working in the efforts to reduce its use to zero.
I was a 16-year-old sweet, innocent, naive country girl in the Wairarapa, living it up and raging and having a good time. Then my boyfriend had a car accident and broke his neck. He ended up in hospital. That had an enormous effect on me as a young girl. I was going to become a nurse and I was going to go and fix everything, him included.
I began working in a large institution in Levin in 1976, working with people with intellectual disabilities and mental illnesses. My whole professional life I’ve worked in healthcare – in frontline work, management, leadership, and consultancy.
Nine years ago I had a mental health event.
It was just an awful experience. Being taken into seclusion is absolutely awful, scary and daunting. No control. You have no control and you know you can’t do anything.
I was mentally unwell and I was very confused, disorientated, lots of thoughts going on. I was quite manic and quite aggressive with it. I was just fighting everything. You just want to fight everything. So you do fight everything.
I grabbed out and I lashed out and then I don’t remember much else. The next thing I remember is sitting on the bed, rocking, and singing to myself.
Years later, I read the observational sheets of myself in seclusion where they wrote that I was rocking and singing, and I cried and cried.
That sense of isolation, that sense of hopelessness, that sense of needing to soothe yourself. All of those sorts of feelings come when I think about it. I can’t stand hearing keys rattling, because that to me is a sign that they’re coming to open the door. You know, they come in teams to open the door to make sure that you don’t attack them.
It’s not a good memory to have. I want to try and stop it from happening to somebody else.
– Jenny Fenwick, 65, registered nurse

Jenny Fenwick’s seclusion event happened roughly around the same time a report (that media called “scathing”) was published by the United Nations Committee against Torture. The report expressed concern at persistent use of seclusion in New Zealand mental health facilities “for the purposes of punishing, disciplining and protecting, as well as for health-related reasons” and recommended we address it.
Outrage, complaints, and calls for change in use of seclusion in New Zealand have recurred in the media through the years. In 2022, the Ombudsman wrote, “seclusion is a serious intervention with no therapeutic benefit and potentially harmful effects on patients. It concerns me greatly that reducing and eliminating its use seems to be making only slow progress, despite my regular calls for it to be stopped.”
Seclusion also has a racial bias – Māori have historically been more likely to be secluded, something the UN committee notes. In 2017, despite representing only 17% of the population, Māori made up approximately 31% of all people admitted to adult inpatient facilities, and, compounding the inequity, nearly half of the total number of inpatients secluded were Māori.
This is, sadly, in line with other countries around the world who seclude patients too much, and with a racial bias, including Australia and the United Kingdom.
Why are people secluded in the first place?
A person having an overwhelming mental health crisis is often frightened, confused, distressed or sometimes reliving a past trauma. They may vividly feel they are in imminent danger, trapped, hearing voices no one else can hear. So they behave in a way that makes sense with what they’re experiencing – they may shout, try to run away, lash out at people around them. They’re in survival mode and the world is a threat.
In a busy hospital or mental health unit, staff have to make quick decisions with a highly distressed person at risk of hurting themselves or others. Staff may feel they have no choice but to “seclude” the person if other ways of calming the situation and keeping everyone safe haven’t worked. This can be a high-stress situation, often involving a team of four trained staff physically restraining a person and placing them into a seclusion room. It’s meant to be a last resort.
But now that distressed person is alone with their distress in a locked, bare room. They may be frightened, confused, or even feel punished for what is happening to them. Many people who have been secluded describe the experience as traumatising, isolating and distressing. Physical and psychological harm to the staff trying to care for them is also well-documented.
For decades, in some countries, strategies, interventions and consumer movements have attempted to bring down rates of seclusion, with little success in the face of degraded, understaffed, overcrowded facilities and long-established practices in mental health care. Many working in mental health care simply felt, in the face of all these pressures, that reducing rates wasn’t actually possible.
But very quietly, work in Aotearoa, now published in a peer-reviewed journal, has shown powerful results at last.

Zero seclusion – is it possible?
The good news story of Auckland district shows it is possible. Back in 2010, Auckland district had seven seclusion rooms and seclusion was being used for about 3,000 hours each year. In the last five years Auckland district mental health facilities have achieved 22 months with no seclusion. In the six months to October 2024, Auckland district units were averaging more than 200 inpatients a month, and no one was secluded at all.
This result is part of a national project to eliminate seclusion. Mental health care was added to the priorities of our national quality improvement agency in July 2017. Following the UN report and after a good deal of consultation with health care services and the people that use them, our persistently high rates of seclusion were identified in September 2017 as an important problem to try and fix.
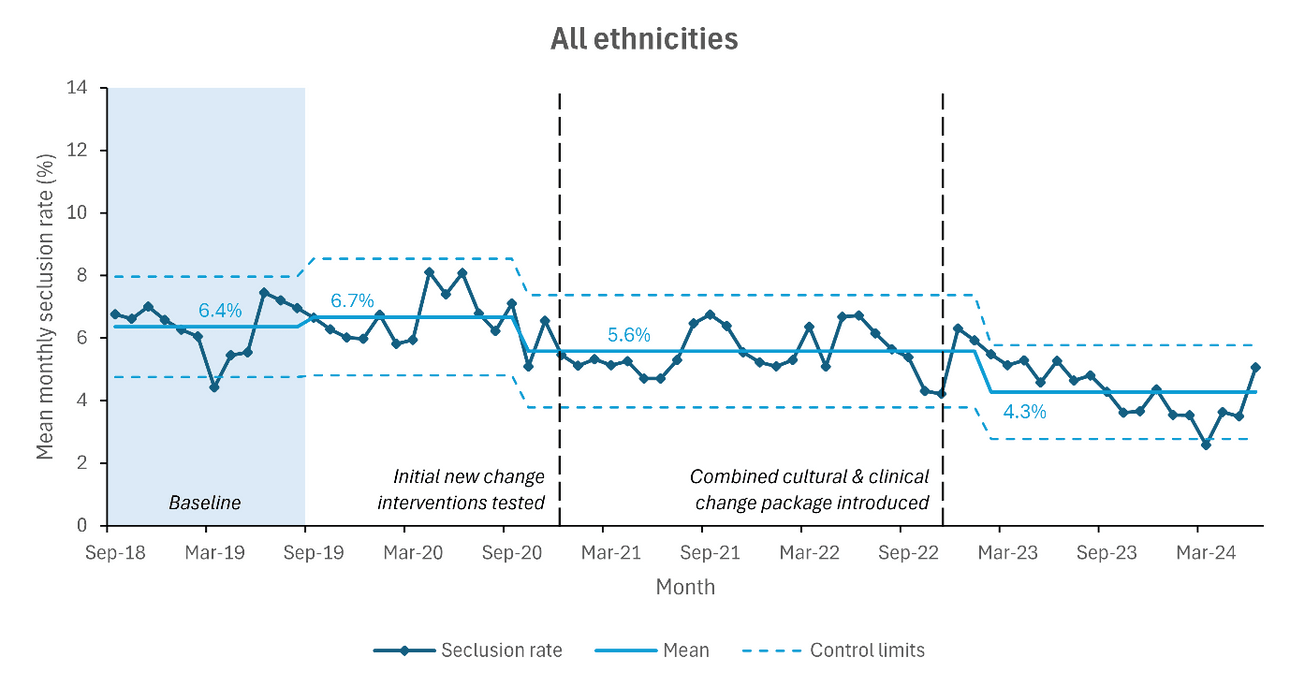
Rigorous data on rates of seclusion were collected in 2018/19 to establish a baseline robust enough to assess whether any improvement had subsequently occurred. At the same time the small national team set about convening mental health teams from across the country, and getting them together with people who’d actually been secluded, along with their families and whānau, to figure out how to bring those rates down. Ultimately, it was decided, the project had to be aspirational. The project itself was named “Zero Seclusion: Safety and Dignity for All”, and the goal was decided, the moonshot: zero.
This new peer-reviewed paper, published in the medical journal Australasian Psychiatry, shows that since that baseline year, the rate of seclusion for all adults admitted to adult, non-forensic inpatient mental health units has been reduced by 33%. This has been maintained since March 2023.
Seclusion of Māori patients has been reduced by 39%.

Seclusion of non-Māori and non-Pacific peoples has halved.

These data don’t represent everyone: the project focused on acute mental health inpatient units, and adult patients only. The data are aggregated from the whole country and behind them are important nuances. Not all facilities are improving at the same rate as others – six of 19 participating districts were yet to show improvement in seclusion rates. However, one third of our hospitals are at virtually zero, and another third are at around 5% and lowering.
What works in Aotearoa to reduce the use of seclusion
So Auckland district and one-third of all New Zealand hospitals demonstrate zero seclusion is possible. What seems to have been key in improving rates of seclusion was the way solutions were found. In a process known as “co-design”, mental health teams and people, like Jenny, who had been secluded worked together with Māori cultural advice to understand, develop and trial alternatives they thought might help.
There was leadership from the center with oversight from clinicians, people with lived experience of seclusion, and respected Māori kaumatua, but there was also local freedom to pursue what works with local people.
New practices – drawing on clinical perspectives, mātauranga Māori approaches, and the experience of people who had been secluded – were implemented and tested in different locations, and local teams measured their results.
These new practices included standardised guidelines for managing acute behavioural disturbance, focused training, cultural support and culturally specific sensory modulation, pōwhiri and welcome into facilities with family if possible, safety huddles and debriefs involving representatives with experience of seclusion, collaboration with police to reduce use of force, involvement of family and whānau at all stages of the inpatient stay, among other strategies.
If something worked in one region it was shared with others, and all successful practices were collected into a “change package”.
Teams were trained and supported to collect more reliable data on seclusion events, with reassurance that data was being collected and used not as a stick to beat them over bad performance, but as a carrot to show them they could get better.
The fundamental shift was in the thinking: that seclusion, even as a last resort, was not an inevitable outcome, but a completely avoidable occurrence. There has been a culture change, and it has spread, if not completely yet. Seclusion is still occurring, and we still suffer from “postcode variation” in where and how much it has reduced, but progress has been made. Zero seclusion is the goal but there is still a way to go.
What these data don’t show is the awful experience that didn’t happen for individual people all across the country – compounded trauma, shame, and, sometimes, actual physical injury incurring longer hospital stays and all the costs to that person and their family, as well as the system.
Jenny’s story
Jenny is planning to retire soon. For 14 years she has been working for a mental health facility as a “consumer adviser” – a person with lived experience who helps teams improve their services. As part of this job she works on the Zero Seclusion project, talking to people about their experiences, reviewing and understanding seclusion events and how they might have been avoided, and working on what could be done differently in future.
“It was just a little thing in my life,” says Jenny, “but such a huge thing, you know? But I don’t want it to be a huge thing in my life.”
“Seclusion could happen to anybody under the current law. While this is the law, we need to do everything possible to prevent it or ensure it’s only ever a rare thing,” she says. “I’d like it to be known that people can do an advance directive that could help prevent this from happening to them in the future.”
An advance health directive is a signed statement that sets out, in advance, treatments people want or do not want if they become unwell in such a way they can’t communicate their preferences at the time. Having an enduring power of attorney (EPOA) can also be a protective factor, she says.
Jenny sings in a band with her husband on guitar. She also plays a big hand drum made from one of their totara trees with a goatskin on top. “I mostly do like to do covers,” she says, and laughs. “I have to admit that I am a bit of a Rod Stewart fan.” But she’s just discovered a new singer-songwriter named Teddy Swims.
“His last name stands for ‘Someone Who Isn’t Myself Sometimes,’” she says and smiles. “Love it.”
She signs off her emails with a quote from the Dalai Lama: “We can let the circumstances of our lives harden us so that we become increasingly resentful and afraid, or we can let them soften us, and make us kinder. You always have the choice.”