


What does the evidence really say about breast-feeding and bottle feeding? And how should we apply that evidence to our own parenting? Dr Jess is on the case.
It was during a breastfeeding class that the terrible “incident” occurred. As I was attempting to get back into my seat after the 10th wee break, I forgot I was 39 weeks pregnant. In my mind I was trying to squeeze my pre-pregnancy body through the teeny weeny gap between the rows. As I executed what was a pretty awkward side-shuffling manoeuvre the guy in the row in front coped a hard smack to the side of his face – with my belly.
For anyone not aware, a full term pregnancy belly is damn hard, being full of baby and all. It would not be dissimilar to getting a basketball to the face (I imagine). The poor guy looked pissed, then mortified and went quite pink. I apologised, felt vaguely embarrassed, then remembered I was 39 weeks pregnant and stopped giving a shit as I collapsed sideways into my seat. Who arranges rows of chairs with only a 30cm gap when your audience comprises grumpy, tired people with huge bellies and no body awareness?
During the class there was talk about latch and hold and there was quite a lot of giggling for a room full of grown adults. Off we all waddled into the abyss of parenthood, confident that the “rugby ball” hold was under our very loosened belts.
And then it all went to hell in a hand basket. It turned out that breastfeeding – that natural wonder of the universe – can be a total bitch. While some decide to breastfeed and find it a straightforward and positive experience and others feel totally OK about using formula from the get go, I suspect both of these are fairly rare subgroups.
For many, if not most new mothers, there is a real struggle involved to start and maintain breastfeeding, with many having painful and negative experiences. There is pressure to breastfeed for some, pressure to give up for others. Some parents who use formula to supplement breast milk do so in secret because if you are in fight club you never talk about fight club. Others find the decision to stop breastfeeding before the recommended six months unbearably guilt ridden. This is really not cool.

So where does the truth and the science lie on breastfeeding?
Is it as critical as we are lead to believe? Are the approaches the health system takes to support breastfeeding the most effective ones? Could we be doing harm with our current approach? And like many things in the maternity system, how can we respect women’s choices (to and to not breastfeed) and not treat them like idiots or infants?
Is Breastfeeding Better?
Lets talk about what we know about breast milk versus formula milk in high-income countries like New Zealand.
Short Term Benefits of Breast Feeding In Countries like New Zealand
The science is pretty clear that exclusively breastfed babies don’t get as ill over the short term as those who have mixed feeding or all formula feeding.
The benefits of breastfeeding over formula in the short term are significant protections from infectious diseases such as gastroenteritis, respiratory disease, and otitis media (middle-ear infections). These are quite serious diseases, especially for babies. Breastfeeding confers greater protection against sudden infant death also [PDF]. The less formula a baby gets and the longer they are breastfed the greater protection they have. For premature babies exclusive breastfeeding is particular good at protecting them from something called necrotising enterocolitis – a disease of the gastrointestinal tract [PDF].
If you are a parent who cannot or does not breastfeed the science may be quite difficult to hear when put this way. We need to consider whether this particular information is what we should focus on to encourage breastfeeding.
Regardless of that, it is useful for those in the health system to know this stuff.
What about the benefits to women over the shorter term? High quality evidence tells us the more you breastfeed the less likely you are to get your period back while breastfeeding (bloody win that!). There is however, no clear evidence that breastfeeding is linked to maternal depression or postpartum weight change. So some of the stuff that is talked about there is just not supported by great evidence.
Long Term Benefits of Breast Feeding in Countries Like New Zealand
The current high quality evidence tells us that breastfeeding reduces the chance of a child getting type 2 diabetes later in life and decreases by 13% the chance they experience overweight/obesity issues as a child and young adult.
There is no association between being breastfed and cholesterol or blood pressure over the long term.
Given these are long-term health issues the science on this is always undergoing review.
For women over the longer term, high quality evidence tells us that breastfeeding offers some protection against breast and ovarian cancer. There is however, no evidence that breastfeeding is linked to bone strength in women.
What about long-term effects of a mixture of formula and breastfeeding?
A high quality systematic review tells us that if we compare exclusive breastfeeding for six months with exclusive breast feeding for three to four months followed by a mixture of formula and breast milk there is no reduction in rates of allergic disease, no effects on a child’s growth, no differences in being obese, or in their intelligence or behaviour.
In other words the long-term benefits don’t appear to change based on the length of the exclusivity.
Summary of the science on benefits
So if you take all this science there is a good case to be made for encouraging and supporting six months of exclusive breastfeeding. And this is probably why the World Health Organisation recommends it as a goal. There are more wins in the short term than the long term, but generally it is a good reason to support breastfeeding in ways that work for women and families (heavy emphasis by me).
*
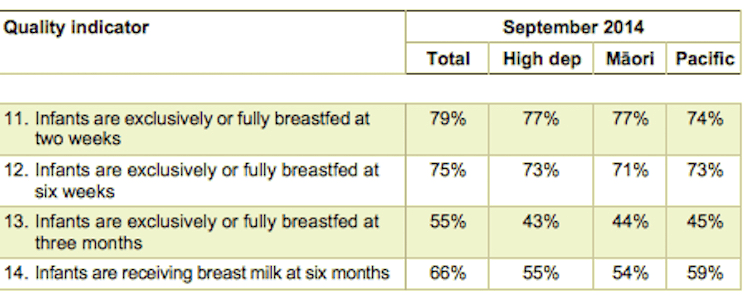
So how are we doing in New Zealand on breastfeeding rates?
Below are Ministry of Health figures, and these represent an increase from recent years, but we could do better especially for our most vulnerable children. “High dep” means children who live in poor communities (“high deprivation”).
How do women feel about feeding their babies?
Oddly, I could not find a study that gave a representative view of women’s experiences of breastfeeding in New Zealand. I say oddly, because if breastfeeding is such an important health goal why don’t we know more about New Zealand’s women’s experiences of either doing it or not doing it?
Perhaps there is some representative data out there that someone could point me to? Nevertheless the studies I could find do give us an understanding of some of the experiences women have, and for some women at least the current culture of breastfeeding is not all that awesome.
In a study of some breastfeeding mothers in Dunedin, women who reported feeling embarrassed about breastfeeding in public were more likely to breastfeed for a shorter period. Shame associated with feeding a baby is not a good thing.
In another study in the UK, both women who breastfeed and those who didn’t talked about the shame associated with feeding their babies. Women who breastfed reported feeling stigmatised for breastfeeding in public, and those who did not reported a sense of failure for formula feeding.
The authors concluded “both breastfeeding and non-breastfeeding women may experience judgment and condemnation in interactions with health professionals as well as within community contexts, leading to feelings of failure, inadequacy and isolation.”

Are we trading off one aspect of health to achieve another?
Research (and it is not representative of all women) does suggest that the current framing of breastfeeding and formula feeding may be compromising the emotional well-being of some women. With women who formula feed (either fully or partially as a supplement) reporting a lot of very negative emotions and stigma when they do so. Such experiences could in part explain why divides open up between parents who breastfeed and those who do not – negative emotions do not for empathetic interactions make.
Good policy needs to consider the “unintended consequences” and how those consequences may interfere with achieving a goal. Maternal mental health is not something to be ignored; being mentally unwell is a significant burden to parents, their children and our society.
Now it is not clear from the research whether shame and negative feelings about feeding babies is a widespread issue in New Zealand, but the research is enough to raise concerns. And added to many women’s stories the research indicates we need to think very carefully about how we are delivering breastfeeding policy so everyone wins.
What is the best way to encourage breastfeeding without harming women (i.e. being women centred)?
The science of the benefits of breastfeeding and the science of what works to increase breastfeeding rates are very different things. So what works to increase breastfeeding?
What we do know across many health issues is that negatively framing the behaviour (i.e. if you don’t breastfeed your baby will get ill, stop smoking or you will die of cancer, don’t eat KFC it will give you diabetes) is a bit of an arse of an approach and positive approaches based on how people actually think and behave work better. Fear of bowel cancer will never convince me to eat that disgusting horsefood people call quinoa for example.
As a public health geek my pet peeve is when we ask individuals to change their behaviours in order to fix problems caused and exacerbated much bigger issues. In the 1950’s breastfeeding rates dropped as the strong-arm tactics of formula companies grew. Since 1970s changes in society structure (more women working, rising living costs, loss of the breastfeeding culture) has continued to have an effect.
Of course we can always say we just need to teach individuals how to change their behaviour (to breastfeed). Yet it takes a huge effort from both those individuals and the system to achieve a health goal this way if nothing at the higher level changes to make it the easy thing to do. Evidence tells us an individual education approach tends not to work, so seems kind of unfair to the people you are “educating’.
Lets look at educating people to breastfeed. The evidence indicates in countries like New Zealand antenatal breastfeeding education does not have much of an impact.
The systematic review conclusions were “We are still unsure if antenatal BF education is able to help women; at present, there is no good evidence from randomised controlled trials to suggest these efforts to educate pregnant women translate into more and longer BF.”
What about after the baby is born, can we educate them to start?
There is low-quality evidence (which means we need better science to be confident) that health education delivered by doctors and nurses and counseling and peer support by trained volunteers improved the number of women who began breastfeeding their babies. The same review found too little evidence to say whether strategies with multimedia, early mother-infant contact, or community-based breastfeeding groups were able to improve breastfeeding initiation.

For women who start breastfeeding what works to help them to continue?
Lots of support helps. The type that is predicable, scheduled, and includes ongoing visits from trained health professionals including midwives, nurses and doctors, or with trained volunteers. Anyone who has first hand experience of the dedication of community volunteers, lactation consultants and midwives will know how this works. The best support may be those adapted to the needs of women, where they live, their cultural and family life but we need additional randomized controlled studies to know.
Many women also experience problems when attempting breastfeeding: latch, nipple pain, or low supply of milk. I have not reviewed interventions for specific breastfeeding problems, but refer you to the Cochrane Library of Systematic Reviews for trusted information. For tongue tie look at this systematic review, and this one for painful nipples.
What about the big picture stuff?
Lets talk about what we in public health rather tediously call “the structural and environmental approaches” and “Creating a supportive wider environment”. This is about what makes breastfeeding the easy, most obvious option.
One such approach is the WHOs Baby Friendly Hospital Initiative. A baby friendly hospital creates an environment that encourages breastfeeding from birth. To be accredited as “baby friendly” a hospital must take ten pro breastfeeding steps and adhere to the International Code of Marketing Breastmilk Substitutes to get accredited. All maternity services in New Zealand are accredited, so if people don’t follow the ten steps listed in a maternity unit that is a problem.
Regulating how formula companies can market formula is something else we do to create a supportive environment. Formula companies are pretty interested in selling as much product as possible, and do use pretty aggressively and use clever psychological tactics to do so. Regulating them (how they can advertise, to who, where and what they can claim) does improve breastfeeding rates. Regulation means women are free from being heavily marketed at by profit motivated companies when making the choice about how they want to feed their babies. The retail value of the industry will reach USD 70.6 billion by 2019 so you can see where the problem may be…..
Workplace supports
The reality is that many women in high income countries go back to work before babies are six months old. This is especially true for families who are feeling the pressure of rising costs of housing and low paid or insecure work. For many families having a baby can be a trigger into poverty because of the loss of income (we can talk about social policy that can counter this next). Workplaces have therefore become an important place where breastfeeding can be supported.
A systematic review found that supports put in place by workplaces, including providing a lactation space, breastfeeding breaks and comprehensive lactation support programs had positive impacts on breastfeeding duration, exclusivity or women’s satisfaction.
Paid parental leave for longer
Common sense would say that the longer a breastfeeding parent has to spend with a child the easier breastfeeding will be to continue, and the evidence bears this out. In a very large review of the effect of paid parental leave policies on health (distinct from unpaid leave) the authors said this
“In our search, a literature review found that longer maternity leave has been consistently associated with duration of breastfeeding in 4 studies in the United States. More recent studies confirm these findings. A longitudinal study found a dose-response association between length of maternity leave and duration of breastfeeding. The study from Canada found that, following the reform of extending parental leave, the average length of breastfeeding increased over a month for eligible mothers and that the proportion of women attaining 6 months of exclusive breastfeeding increased”
Income support for those least likely to breastfeed
It is clear that women who are better set up in our community, have more wealth, more education, breastfeed more and for longer. My own research on children’s wellbeing and parent’s wealth describes in detail why the children of parents with more wealth do better. When we increase the incomes and belief in the inherent expertise of parents with young children the flow on effect to children is significant, in all areas of well-being, one of which includes the parent and child relationship.
We all want the best for our children (and this includes the choice to breastfeed where possible), but with rising costs, the need to go back to work, and a lack of cash to pay for lactation consultants if feeding doesn’t go well, those on lower incomes do not have the same choices about parenting as the better off in New Zealand.
And what works to reduce stigma of not breastfeeding?
In Norway (a country with very high rates of breastfeeding) they are recognizing the potentially negative outcomes of being stigmatized for formula feeding when a breastfeeding culture is strong. Researchers have suggested that to help women overcome some of the negative experiences associated with stopping breastfeeding that they “…ensure that infant formula is used correctly and to reduce stigma, healthcare workers should have sufficient knowledge about formula feeding and health authorities could provide information about how to prepare infant formula”.
(Editor’s note: Here is a guide to using formula)
This is not evidence of what works, rather it is something to consider exploring further if we are really committed to women-centred care.
A final word
What is the take home here then? What would I say to my new parent self? I would say this:
“OK, breastfeeding is a good thing to do. So if you want to do it advocate for that right and for the support you need to do it, don’t let anyone decide for you. Good on you for choosing something that works for your families’ wellbeing (women do not hear this enough). But if breastfeeding is making life a misery and you want to stop then this is not something to feel awful about. Don’t let someone decide for you. If you have decided this is best for your family, then good on you for making a decision that works for your families’ wellbeing (women do not hear this enough)”
Evidence is not a prescription for living; it is a piece of information to make a decision with. Families, mothers and babies’ health exist within an entire ecosystem of wellbeing and breastfeeding is just one aspect of this. You and your baby are not personally responsible for achieving the health’s system goal to up our breastfeeding rates; you are only responsible for making things work for you and your family. It is the system’s responsibility to pay close attention to what works best to achieve a high rate of exclusive breastfeeding for all, and not rely on a select few approaches that lean heavily on individuals.
Finally, women can support each other for deciding to do best for their overall wellbeing no matter what their choice AND together we all can advocate for better women-centred approaches that work for all women and families based on the evidence of what works.
Dr Jess Berentson-Shaw is The Spinoff Parents resident evidence-based scientist, all-round bullshit detector, and mum. She agitates on evidence and good social policy and believes in the power of honest storytelling. See her full bio and work here.
Follow the Spinoff Parents on Facebook and Twitter.