


A major University of Otago study suggests poorer outcomes for babies born under midwife-led care. Dr Jess Berentson-Shaw looks at the truth behind the headlines.
In this article we are going to talk about some of the bad stuff that happens during pregnancy and labour to babies and women. These things are infrequent in New Zealand, but we are not going to shy away from the reality that they could be more infrequent. Good science requires us to look these things in the eye and ask: Can we stop the bad shit from happening?
For women and their families who have experienced the cruel and bitter side of birth, we recognise the terrible pain and trauma you have gone through. If you do choose to read on know that this piece is focused on what the system can and needs to do better for you and your families, and all women and whānau. All of our aroha to you; your grief does not go unacknowledged. – Emily Writes, Spinoff Parents editor
So you heard some stuff in the news about midwives and doctors and babies and now you are thinking, what the hell?
Recently a new study came out looking at outcomes for babies (not women) under different types of care in New Zealand. The study showed that babies born under midwifery-led care had more complications – for example, they were at greater risk of a lack of oxygen during birth – than those under doctor-led care. This sounds not so great, and may have some of you worrying about your maternity care.
First, let’s be clear that the risk of a poor outcome for a baby is small in New Zealand generally and consequently the differences in outcomes between midwife-led and doctor-led care are also pretty small for babies and mothers. For example, let’s look at the risk to a baby of having a low Apgar score – the measure of how responsive a baby is just after birth – as they were reported in the study:
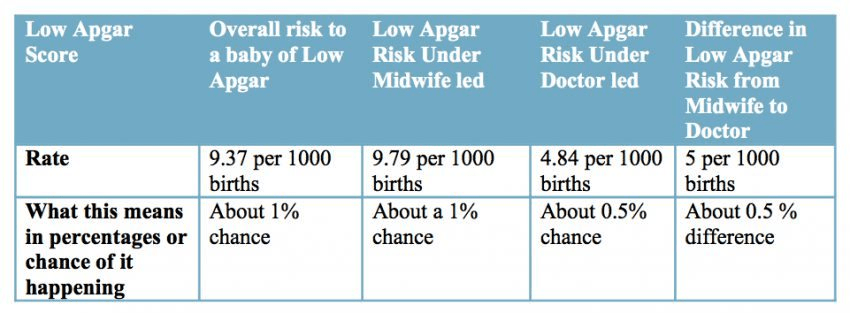
So the risks are small to start with and under doctor-led care the risk becomes a bit smaller. However, once you start to apply that risk to the number of babies born in the country (around 60,000 per year) we can see that there is a problem that we shouldn’t ignore. The impact of these events is very, very real when you are standing in the sterile, wincingly bright and lonely corridors of a hospital contemplating life and death – sometimes before life has even begun. So while from a risk perspective the chance is thankfully small, there is work to be done and we need to acknowledge that.
The good news is that we know from really high quality research overseas that midwifery-led care can actually be better for women than doctor-led care (for example, there are fewer interventions under midwives) and just as good for babies under optimal circumstances. Now we just have to make sure we know what is going on in New Zealand.
I want to use this piece to help explain how the study shows that New Zealand may have a problem with the way its maternity ‘system’ is working. It does not show midwives are the cause of those problems. Rather it points to what many working in the system, like midwives and doctors, and birthing women themselves have been saying for years: that the way our maternity system operates needs attention. So we need to talk about that, but first let’s reassure ourselves that overall New Zealand is a safe place to have a baby.

How safe is New Zealand overall in terms of having a baby?
If you have a baby in New Zealand, by far the most likely outcome is a positive one.
How do we know it is safe? Well our rates of the bad stuff (very technical term that) are very low internationally: comparable to the UK and far, far better than all developing countries and many developed ones tooi.
Is birth risk free in New Zealand?
No. There is a difference between relatively safe and risk free. Expecting all births to be risk free is a big ask and beyond our science and technology right now. Also, delivering (pun intended) a totally risk free birth may well require giving up things we as women and whānau are not prepared to.
And so that bad stuff, tell me about it…
A so-called ‘normal’ birth in New Zealand is what we call a ‘spontaneous vaginal delivery’ without medical interventions. These births have the least impact on women and the health system. So labour is not induced, goes OK (though frankly that feeble little word pain does not even get close to encapsulating the appalling trial by fire that is labour), with no epidural, and ends with an intact baby and mother, a nicely delivered placenta yada yada. Awesome.
Guess how many women have this birth in New Zealand? Oh only about 34% (fewer for a first birth). Perhaps someone really needs to rethink the use of that word ‘normal’?
Below is another table to give you an idea about the rate of various types of not so awesome things happening during and after birth. Keep in mind there are about 60,000 births each year in New Zealand.
| Woman Outcomes |
% of women or babies |
| Labour | |
| Induction |
25 |
| Epidural |
25 |
| Episiotomy |
15 |
| Type of Birth | |
| Unassisted vaginal (with or without labour interventions) |
65 |
| Assisted Vaginal (forceps, vacuum) |
9 |
| Caesarean Section |
26 |
| Emergency |
13 |
| Elective |
13 |
| Baby Outcomes * | |
| Premature Birth (before 36 weeks) |
7.4 |
| Low birth weight |
5.9 |
| High Birth Weight |
2.4 |
| * Ministry of Health does not report other baby outcomes on a national level without a special request. | |
While our rates of perinatal death are sinking, interventions in births are rising. In New Zealand, for example, our total caesarean rate is 26% and it rises every year. The World Health Organisation says the optimal rate is 10-15% and after this risks to women and babies actually rise. People do wonder why we count epidurals as an intervention. An epidural is not a pain killer in your back. Rather it works by a totally different mechanism. Anaesthetic is injected into the spine and numbs the pain nerves as they enter the spinal cord. While overall very safe, they are a serious medical procedure and have small but serious risks associated with them including breathing issues, spinal cord and nerve damage.
Epidurals also change how women give birth. Without feeling in nerve endings, women cannot move around much during labour: walking, changing position, rolling around, shouting at people (!), or helping with positioning and moving the baby through her pelvis. It also helps women to actively cope. Knowing when, how long and how much effort to put into pushing can also be difficult as women cannot feel the baby move through the cervix and vagina. Ultimately women who have epidurals are more likely to have other interventions including episiotomies and forceps and caesarean sections.
Are some women and babies experiencing these poor outcomes more than others?
Yes, some women and babies experience these outcomes at a greater rate than others, and this is often because they have more ‘risk factors’ present. Science gives us a good lead on preventing or mitigating many of these risks. For example, we know diabetes in pregnancy is a big risk. So we first try and prevent it developing, then we try to identify it early, then we try and manage it well if women do develop it. We monitor their babies. Finally we may intervene.
This clinical stuff is one thing, but other problems arise when factors that really should not be putting women and babies at risk, do. A woman’s economic status, her education, her ethnicity, or her maternity care choices are not things that in an equitable public health system should change a woman and baby’s risk. Yet in New Zealand many of these things do increase risks. If such things are determining outcomes, we call them “potentially avoidable”.
For instance, the Perinatal and Maternal Mortality Review Committee (PMMRC) has found consistently year on year: “The proportion of potentially avoidable perinatal related deaths [babies who die in pregnancy, labour or the month after birth] increases with increasing socioeconomic deprivation…“

So we could do a better job at avoiding poor outcomes?
Yes. Especially where those factors like ethnicity, lack of material resources, and where you live are conferring risk.
As the PMMRC points out pretty much every year in their reports, the increased risks of perinatal death they observe in those from poorer communities are “due to increasing contribution from barriers to access and/or engagement with care”.
We should not shy away from how economic and social inequalities (and let’s call it for what it is – racism) determine outcomes for women and children in this country. We need to look that nasty reality in the eye more often and do way, way better.
Of particular interest is whether the care women receive is an additional source of risk. Clearly the intention is that maternity care should reduce risk and the inequalities that exist. Care should be targeted to those at greatest risk in a way that works for them (i.e. patient centred) and be of sufficient quality to mitigate their risk. While the onus is not on the health system alone to solve wealth and ethnic inequalities, the function of a public health system is as a buffer against these risks.
So let’s look now at the role that maternity care might play in this particular issue: conferring or mitigating the risks of birth.
The model of maternity care in New Zealand
In New Zealand you can choose to have midwife as your Lead Maternity Carer (LMC); the government pays for this for you. You can have a self-employed (community) midwife, or a hospital-based midwife team. There are a few general practitioners (GPs) that still deliver LMC care under the public health system.
If you need a doctor because you are at additional risk, you may be based under a specialist team at a hospital. In some cases you can choose a shared care arrangement between your community midwife and this team. Such scenarios are also free. These arrangements are complex and the data does not always capture them well.
Pregnant women can also choose to have a private obstetrician. There is a charge starting around $4000. Usually midwives who work with the obstetrician will deliver part of the care.
Up until the 1990s in New Zealand maternity care was provided by GPs, obstetricians, and midwives. After a big shake up – designed to reflect the normal process of most births, improve the cost effectiveness of the system, and still give women ‘continuity of care’ (the same person caring for you throughout pregnancy and labour) – midwifery-led care has become the norm. GPs moved out of the business because the new funding arrangements made it unsustainable for them to continue.
Who gets what care in New Zealand?
Most women (around 85%) use midwife-led care; they want it and need it. Great.
About 0.5% of women use a GP.
Some women get funded doctor-led care/shared care from a specialist team because they need it. Also great. This data is hard to find as often a pregnant person’s first registration is with a midwife and they may continue in some capacity with them.
Some pregnant women want doctor-(obstetrician)-led care so they pay a surcharge (on top of the funding the Ministry of Health provides) for it. About 6% of women use a private obstetrician, according to the Ministry of Health. Obstetricians add choice to the system and it seems fine unless women getting this doctor-led care (and the new study tells us these women are wealthier, older and more likely to be of European/Pākehā descent) are in effect paying a top-up to get better outcomes. Then we have a problem. That is not how it is supposed to work in an equitable health system, which is what we, in theory, have.
Some women get no care. Around 9% of women are not registered with a maternity carer – they may have received care from hospital midwives but they also may have received no care at all. These women are more likely to be Pacific and Indian women and, again, those living in the most deprived neighbourhoods.
Hmmmm.
Is a doctor-led model of care better for women and babies?
Not according to research. Midwifery care is just as good, if not better, than doctor-led care for low risk pregnancies. The great news is that a recent systematic review of high quality randomised controlled trials (this is where women are randomly assigned to different types of care, so you know that there is nothing about the particular characteristics of the women that determine either what care they receive or the outcomes they experience), showed that women do BETTER under midwifery care (fewer epidurals and episiotomies) and babies do just as well. Fewer interventions for women are a good outcome too; we are working hard in the system to avoid the cascade of interventions.
Knowing that babies can be just as safe under either model of care is fantastic because midwives are here to stay and are an important part of the system. They matter to women who see birth as a normal event, not a medical one, and they help keep costs to the New Zealand public lower, so money can be spent on other health needs.
Does this research show that in New Zealand the implementation of the maternity model has gone awry, and that paying for doctor-led care buys better outcomes?
The trials showing midwifery care can be just as good for babies and better for women were delivered (see what I did there) under optimal conditions. Like all of these studies, the trials were run by dedicated passionate scientists, who devote years of their lives to the perfect test of an intervention. The realities of how a model works in real life, once all the politics and problems of health systems start to play out, can look a bit different.
So let’s go back to what new research tells us about maternity care in New Zealand
Shockingly, this is the first time a proper big look at outcomes for babies (not women mind you) based on the model of care they receive has been undertaken in New Zealand. And it is simply a very first step. The research should have been done a lot earlier by those responsible for the policy changes in the first place, and not left to a group of interested and dedicated midwives and doctors.
The study was a retrospective study, which means it looked back in time at a whole lot of births and tried to see if there was a relationship between models of care and baby outcomes. It is called a retrospective cohort study and looks at the ‘aetiology’ of a condition – i.e. what is happening to whom, how, when, and under what circumstances. To get technical, a retrospective study is not the optimal way to look at aetiology; it is best to do this with a prospective study (which I discuss below). But that does not mean the study is flawed, only that it is a first start with what data was available.
The authors know there are many other things (not just model of care) that can explain poor outcomes for women and so they either removed high-risk women from the study altogether (i.e. those under hospital specialist care and women who did not have a maternity carer) or used statistics to make all women ‘equivalent’. So they ‘controlled’ for ethnicity, relative wealth, age, smoking status, body mass index, among other things. They found that women under midwife-led care at the start of their pregnancy (but not necessarily during labour, as they were limited by the data that is routinely collected by hospitals) had increased risks of having babies with certain complications compared to those with doctor-led care.
Of course the researchers cannot entirely control for all the factors that may explain why women under midwife-led care may have poorer baby outcomes, but they did a pretty comprehensive job. There remained a connection between being registered with a midwife and elevated risks of some poorer baby outcomes.
Does this tell us that it was a low standard of care by midwives that caused these elevated risks? No, we don’t have the right data to tell us that. And the authors certainly do not claim that that is what their study shows. These are good scientists – they know what they can, and cannot, do with such results. What they did say is this:
“It may well be that midwife-led care is optimal within the context of well-organised systems. However, there is an urgent need to establish which aspects of those systems potentially make that care more, or less, safe [in New Zealand].”

So given an issue has been raised about midwifery-led care how could we find out what is going on in the system?
First, we need to not bury our heads in the sand and say no no no this is a bad study and it is not not NOT true. Even if you believe the results to be part of a sustained attack on midwives, the next step is to invite further exploration and see if the findings hold with a different approach.
In terms of research we would now want a ‘prospective study’ to confirm if there are differences in care. That is where we identify women at the start of their pregnancy and then follow them through their pregnancy actively collecting the data the study needs (not just what hospitals happen to collect, as routine data is not great at answering in-depth research questions and can be subject to politics). We note what kind of care women have, information about them, and their pregnancy. We gather specific information on issues that we hypothesise may be at play, like clinician experience, transfer of care and communication. We then look at outcomes both the mothers and their babies experience. We look again to see if the differences in care are replicated and this time we have more detail to see what is at play.
Such an approach is accepted and expected in other areas of the health system. For instance we have spent a lot of time using both retrospective and prospective studies of bowel cancer surgery to look at how care factors influence outcomes for patients. We have seen, using these types of studies, that the caseload, experience, and expertise of the surgeons delivering care matters in patient outcomes. On the basis of this research recommendations have been made as to who should do surgery, what their caseload should be, and what training they need. The patients and the clinicians benefit from such changes and survival rates from colorectal cancer treatments have improved.
It was not an attack on the clinicians in the system – it was simply evidence-based quality improvement.
So there are four things the Ministry of Health can do right now
- Pay for the above research to be done, and done well.
- Compare the optimal models from the existing research on models of care with what we are delivering in New Zealand right now.
One way to do this is to look at what we call evidenced based guidelines (here is one from the UK) and see how our current practice lines up. There are exciting developments internationally with things called “bundles of care” where every patient MUST have a specific set of clinical activities done for them and signed off. This takes away the onus on any one professional group and makes it simply about delivery the care a patient needs to ensure optimal outcomes. New Zealand has a pretty slack approach to ensuring health delivery is lined up with evidence-based practice. The government stopped funding the development of most evidenced-based clinical guidelines some time back, and even then we were not particularly great at making sure those in the system adhered to them. So much for an evidence-based culture.
Another way to do this comparative work is to look at similar models internationally. Denmark and the Netherlands both have midwifery-led care. What are their outcomes like and what do they do the same and differently? How do they ensure high quality care? In Denmark, for example, they video emergency events and then seek permission to review them to see how the team has worked together as part of good clinical practice.
3) Compare the care factors in births that went wrong and those that went right.
We have some leads on this already.
When researchers have reviewed births where things went wrong for women and babies in New Zealand, the issues that have been highlighted include the need for clearer evidenced-based guidelines for serious events for all staff, better planning, enhanced supervision of junior staff, and enhanced communication in multidisciplinary meetings. Perhaps these things also occur in births that go right too, perhaps they don’t. We need to know to implement change.
4) Ask some hard questions about how system is arranged. Here are some (many) for a start
- Is the current payment system set up to create disincentives for optimal shared care?
- Are we putting the right amount of money and support in the right way into midwifery services?
- Are we putting the right amount into specialist provision?
- Are midwives getting the optimum training and support following training?
- Are obstetricians being trained in the context of how care is delivered in New Zealand? i.e. “shared care” not “doctors are the boss” care.
- Could we use GPs more effectively especially for those women who are harder to reach and at greater risk?
- What can be done to break down hierarchies, improve communications, and address the issues that exacerbate hierarchies?
- Most importantly what can be done to address the massive inequalities in outcomes between different women and babies?
And let’s face it, none of the issues raised are any great surprise to many women and their families
Research tells us that women are very aware of how the power dynamics (between midwives and doctors, and junior and senior doctors) play out in less than ideal ways during their pregnancy and labour, and that these influence the care they receive.
In my many conversations with women about birth most have highlighted some aspect of their care, whether it be about midwives or obstetricians that has created a level of disquiet, even alarm.
No profession is innocent here. Not doctors, not midwives, not those in policy.
What next then?
“Randomise everyone, everywhere.” That’s what Ben Goldacre, the guru of good science/ bad science, argued recently on his blog. His point was that good scientific principles need to be applied to determine ‘what works’ when we implement new health services within our systems, not just when looking at ‘what works’ in the lab.
Whatever research reveals about the maternity system, and whatever is decided to be done about it, needs to be tested and trialled and measured properly. There are clever ways to do this without women missing out on high standards of care. Those in the Ministry of Health should understand good evidence, and if the government really supports quality evidence, they can be leaders. Policy innovation is one thing; not following it up with proper evaluation is far, far too common in this country.
The takeaway message for parents
Having a baby in New Zealand is safe no matter what model of care you choose, compared to other countries just like us. The rate of perinatal death (babies dying before, during, and after birth) has been on a steady decline for many years. Women dying in birth is such a rare event that it is hard to create statistics on it.
But birth is not risk free and it is a massive life event; being mentally prepared and feeling supported is important. If you feel uncomfortable with the care you are getting then do not hesitate to change – it is your legal right. Continuity of care is important but that can also come from a support person, friend, mother, or relative that travels your journey with you. So draw on your support network if your maternity carer needs to change.
The research tells us that midwifery care is just fine for babies, and obstetrician care just fine for women under optimum conditions. If you feel conditions are not optimal, then find someone who can advocate for you. Offer to be an advocate for those who cannot advocate for themselves. Demand better of the system. Demand that Government support all clinicians in the system to deliver optimal care and all women and babies to receive it.
The takeaway message for midwives, obstetricians and policy makers
New Zealand loves to innovate in policy. We hate to evaluate properly. New Zealand has a unique and in many aspects positive maternity care system. But it is not enough. We need to know if it is structured in the optimal way to deliver the best outcomes for all.
I have taken an equal-opportunities approach to potentially offending all groups involved in maternity care – doctors, midwives and the Ministry of Health – because all professional bodies need to shoulder responsibility for making the system work better for women and their babies. We should all look closely at our motivations for wanting to believe or dismiss a piece of research out of hand. We need to welcome rigorous and fair inspection to achieve better outcomes for women and babies. The issues will not sort themselves out when all fingers of blame are pointed elsewhere and people continue to furiously patch protect. However, we also need to recognise how power dynamics work in such systems and as such, the onus is on the Ministry of Health to be the dispassionate facilitator of best practice and not sweep this issue under the carpet.
Dr Jess works at the Morgan Foundation public policy think tank. She agitates on evidence and good social policy and believes in the power of honest storytelling. See her full bio and work here.