
More needs to be done to help those at risk, so let’s get the facts straight, says Jess McAllen.
This story first appeared on The Wireless. Read the rest of the series here.
Suicide is a tough issue to talk about. With 606 suicides last year, there’s no doubt more needs to be done to support those most at risk. And the best solutions are going to come from having an informed debate.
It’s time to bust some myths about suicide in New Zealand.
Myth 1 – Suicide affects all parts of society equally
Anyone from any background can feel suicidal, and die by suicide. But it is important to acknowledge that some groups of people simply are at higher risk than others.
Mental Health Foundation chief executive Shaun Robinson says we need to acknowledge this if we are ever going to tackle the common drivers of poor mental health and suicide. For youth aged 15–24 years, the number of suicides was four times as high in the most deprived areas compared with the rate in the least deprived areas.
“Māori are nearly twice as likely to die by suicide as non-Māori, and men three times as likely as women. People who are living in poverty, people who identify as LGBTI, people who are isolated, dependent on drugs or alcohol, discriminated against or excluded all have specific life experiences that mean they are at higher risk of suicide.
“If we want to make a difference in our suicide rate, we need to address the specific factors that create this risk.”
Myth 2 – The law gags the media from talking about suicide
Just over a year ago, the Coroner’s Act was amended and loosened the laws around suicide reporting. Many journalists said the change needed to happen in order to bring down the rates.
For the past year journalists have been able to report on suspected suicides before they are officially ruled a suicide, but are still barred from reporting method or location of death if it identifies method.
Suicide contagion (the idea that certain types of publicity around suicide can lead to copycat behaviour) is not about everyone reading an article and suddenly having the desire to kill themselves. It is a proven fact that vulnerable people who are experiencing mental distress can be negatively impacted by constant sensational suicide coverage. For some reason being told to talk responsibly about suicide has been conflated with “never talk about suicide”.
While there are media guidelines for reporting on suicide, a study on suicide contagion in New Zealand, released late last year, (which interviewed New Zealand journalists and editors) found that they were largely disregarded.
The author, Craig Colhoun, noted: “participant criticisms of contagion research may also reflect their desire to believe that their daily reporting does not harm readers. As a result, it is likely that participants are automatically primed to negatively interpret and oppose any research conclusions supporting suicide contagion.”
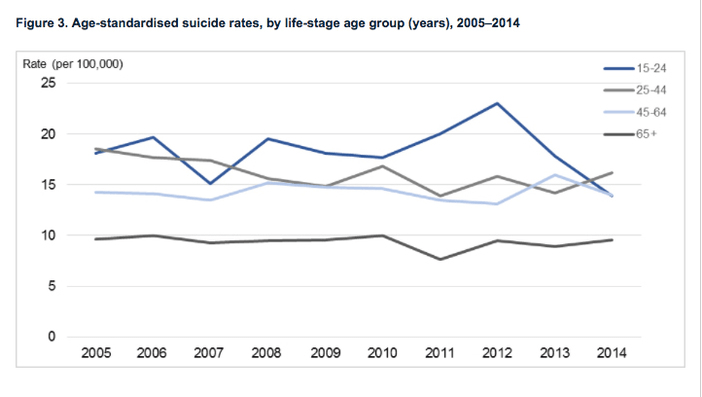
Myth 3 – Our youth suicide rate is the highest it’s ever been
Our youth suicide rate peaked in 1995 with 156 deaths in the 15-24-year-old age group (at a population rate of 28.7 deaths per 100,000). The information is available here (data tables, table 1).
The most recent spike in youth suicides was in 2012 (148 suicides at 23.7 deaths per 100,000). The youth suicide rate has been on a downward trend since then. The provisional figures from 2012-2016 also back up the downward trend in youth suicide.
We do, however, have the worst youth suicide rate in the OECD.
Our worst general suicide rate was in 1998, when there were 15.1 deaths per 100,000. The provisional figures released last week (which aren’t finalised) put last year’s rate at 12.64 per 100,000.
Here’s a breakdown of the age-specific suicide numbers as per the provisional report released by the Coroner each year:
AGE BRACKET OF 14 YEARS PER GROUP
2016 release
10-24: 119
25-39: 161
40-54: 157
55-69: 99
70-84: 37
85+: 6
2017 release
10-24: 130
25-38: 153
40-54: 171
55-69: 104
70-84: 34
85+: 14
Myth 4 – The true suicide rate is three times higher than reported
This is a very serious claim with “no basis in reality”, says Robinson.“Even if every sudden death in New Zealand was caused by suicide, there are not enough sudden deaths even to double the suicide rate, let alone triple it.”
He thinks the misunderstanding comes from the fact that suicide is a legal term, and coroners need to be able to say with reasonable certainty that a person did intend to take their life. “If the death was an accident or the person who died could not be found to be responsible for their actions, it won’t be ruled a suicide,” says Robinson.
But even if the death is ruled as self-inflicted rather than a suicide, it is still reported in the provisional suicide statistics put out each year. By the time the official Ministry of Health suicide statistics come out (usually a couple of years after the Chief Coroner’s suspected suicide statistics, because there are only so many coroners to work individual cases) the (on average) 30 or so deaths that are not legally ruled a suicide will not be included.
Myth 5 – Deaths are not considered suicide if there are drugs and alcohol in the person’s system
The official data released by the Chief Coroner has a breakdown of the percentage of people who kill themselves via a drug overdose.
“Often, people in extreme emotional pain use alcohol or drugs to cope with what they are thinking or feeling. Many suicide deaths occur when someone has been drinking or has drugs in their system,” says Robinson.
The Foundation is also concerned that discussion around what method “counts” means people will attempt those methods in order to spare their family the shame and stigma of a suicide death.
The Suicide Mortality Review Committee Report, released last year, found that around half of Māori youth tested positive for alcohol at the time of their death.
This story first appeared on The Wireless. Read the rest of the series here.
WHERE TO GET HELP WITH MENTAL HEALTH
Need to talk? Free call or text 1737 to talk to a trained counsellor, anytime.
Lifeline: 0800 543 354
Suicide Crisis Helpline: 0508 828 865 / 0508 TAUTOKO
Depression Helpline: 0800 111 757
Samaritans: 0800 726 666
Youthline: 0800 376 633 or email talk@youthline.co.nz
Healthline: 0800 611 116
The Society section is sponsored by AUT. As a contemporary university we’re focused on providing exceptional learning experiences, developing impactful research and forging strong industry partnerships. Start your university journey with us today.