
Dr James Jap regularly watches people die. He talks to Michelle Langstone about how working in palliative care has shaped his outlook, his family, and his wardrobe.
James Jap had never seen anyone die until his fourth year of medical school. On an overnight shift with St John’s ambulance, he was called out to the middle of the Otago countryside to see a man who was very unwell. “We ended up doing CPR and trying to resuscitate this man in the back of an ambulance at 3am in the morning. It was all dark. I didn’t know where I was. It was quite a chaotic, traumatic experience.” Jap, now a palliative care physician at South Auckland’s Totara Hospice, says it was a formative moment in his early career.
“It was just like whoa. OK – this is sort of like what you see on TV! But on TV people come out alive and they’re fine, but this guy wasn’t fine, and he died in front of me. That was the first experience of a death that I’d had.”
It wasn’t until a few months later, on a morning shift at Otago Community Hospice, that Jap realised the impact of that night out in the dark. He arrived for his clinical rotation at the hospice in the moments after a man had died. “Everything was calm and peaceful. The chap looked nice, there was almost a hint of a smile on his face. He just looked serene. But his wife was the one that I looked at, because she was good. Her husband had just died but she was OK, and it was all very calm and collected.” Jap says that’s the moment he got the first spark of an idea to become a palliative physician. “I said, ‘OK, maybe death doesn’t have to be so traumatic and so chaotic. Maybe there is another way. It doesn’t have to be so stormy, so frightening, and so scary for everybody.”
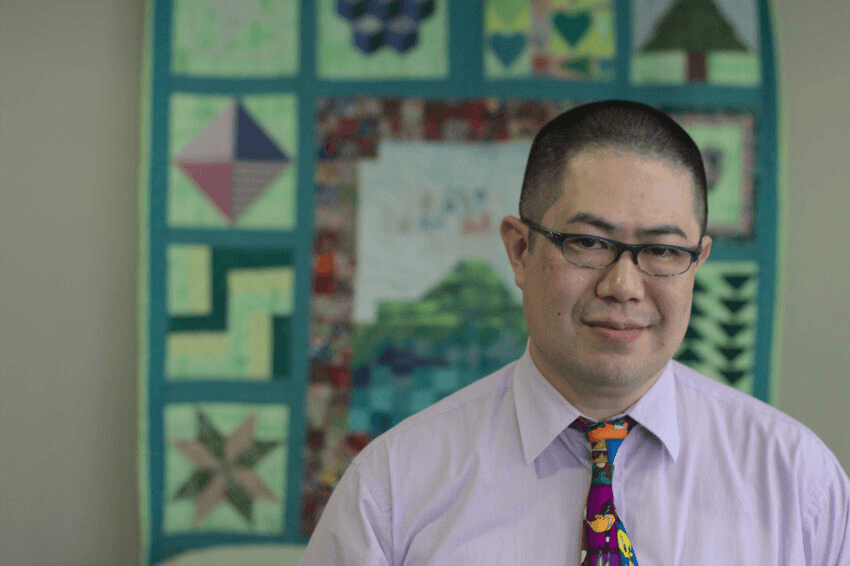
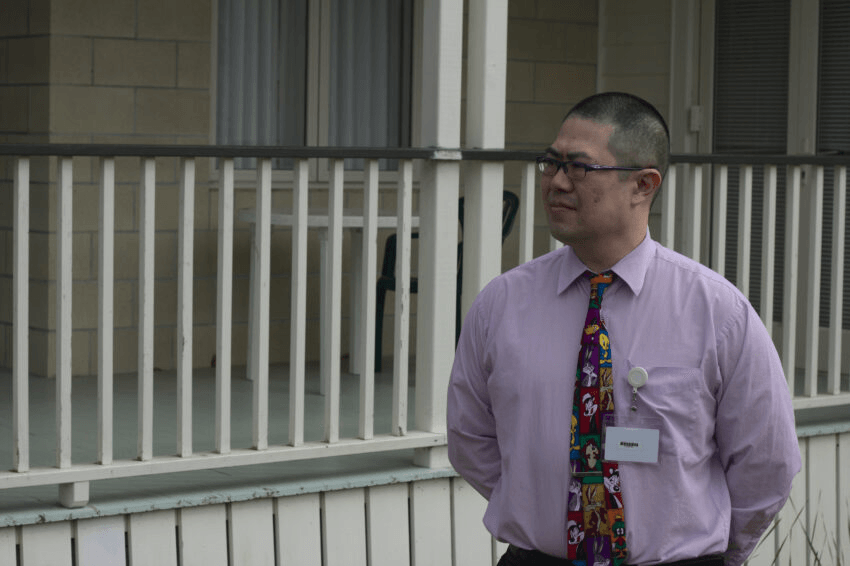
Totara Hospice sits on a leafy site in Manurewa. It’s a gentle old building with wraparound porches and lots of sunlight. I meet Jap on a break in his rounds, in a quiet room where patients and their families can come to sit and contemplate. The windows in the corner are luminous pieces of stained glass, and they throw jewel-coloured shapes onto the carpet in bright segments. They match the tie Jap has on, a mosaic pattern of Looney Tunes characters: Daffy Duck, Tweety Bird, Bugs Bunny. Jap is a quiet man, tidy and economic in his movements. He speaks in a low, steady voice that is both calming and clear. He’s been a doctor for 21 years, and a palliative care specialist for 12.
I ask Jap if there’s a misconception around palliative care in the community, and he pushes his glasses up his nose and looks very tired for a moment. “We’ve become a death-defying society because of modern medicine, and because the conversation about death and dying isn’t out there in the public. People don’t talk about it.”
Jap says 70 years ago, before the advent of antibiotics, death was much more a part of everyday life; but now modern medicine and surgery means it’s not. “We have 30-plus-year-olds who’ve never been to a funeral because nobody [they know] has actually died before. We’ve made it so foreign to our day-to-day life that we’re afraid of it.” What’s missing, he says, is the understanding that the end of life can be profound, and beautiful. “It’s not just about the final dying process, it’s about enabling the person to be as living as possible given their situation.” Jap says it’s not uncommon to see about 70% of patients come through for a short visit, and then grow well enough to go home again. Hospice is not just a place people go to die, but a wraparound support service.
“When a person is feeling unwell, if they’re being suppressed by their symptoms – like pain or nausea or a combination of things – they’re not feeling like themselves. So my job is to try and calm those symptoms down. Those symptoms are like a cloud that’s covering up the true light of the person within. My job is to get rid of some of those clouds so that person can shine through again.”

Palliative care in New Zealand is potentially on the cusp of change, with the public voting on the End of Life Choice Act in this year’s election. I ask Jap what that means for Totara Hospice, which hasn’t come out alongside Hospice New Zealand to denounce the act and have instead stated their intention to work alongside the law. “At the moment our care is very pro-patient choice. It’s patient-directed care, it’s patient-centric care, and that’s not going to change no matter what happens to the law.”
It’s the great unknown for palliative care, and it’s obvious from the way Jap measures his words that he’s not quite sure how it’s going to be for the doctors and nurses he works with if the act goes through. “Our staff may not be doing the administration of assisted dying ourselves. But we’re going to be looking after people up until that point, and after that point, which is what we do anyway. So is it going to change the care that we actually provide? I don’t want it to.”
Critics of the act are worried that health inequities may see vulnerable patients choosing to end life early rather than be a burden to their families and community. There are concerns about the accessibility of palliative care around New Zealand. Because hospices rely heavily on charity, the services aren’t as widely available as they should be. Totara receives a proportion of their funding from Counties Manukau Health, and the rest they make up for in donations – roughly an additional $4 million is required each year in order to provide a service that’s free for everyone. Totara has nine beds in its inpatient unit, and approximately 370 patients it visits in the community.
It sounds like a decent amount, but it’s still not reaching everyone who needs help, and health professionals have expressed concern that people unable to access palliative care support may choose to end their lives prematurely. I ask Jap if he’s concerned about patients being coerced into dying early and he reiterates that, according to the bill, clinicians must check for signs of coercion during conversations about assisted dying. He’s careful to stress it’s his own personal opinion that coercion would be unlikely.
Totara caters to an exceptionally diverse South Auckland demographic. “There are so many different cultures, and I really love it that on a standard ward round, in one room I’ll have someone from Tonga, the next room Samoa, next India, then Yugoslavia,” grins Jap. He adjusts his tie and leans forward, resting his forearms on his knees as he enthuses: “We have something to learn from all these different cultures, and we need to be much more culturally aware and responsive.” Totara Hospice is focused on inclusion, and alongside Mary Potter Hospice and The Māori Medical Practitioners Association, it’s created a Māori-led palliative care model that centres on the concept of whānau as a chief tenet of care.
“You talk about institutional racism and the health disparities for Māori and Pākehā, and the rest of New Zealanders. That’s something we are trying to address in palliative care. We launched Mauri Mate which is a palliative care framework designed by Māori, for Māori. So we’re going to try to address the equity gap.” Jap gives his broadest smile, which is still very modest. It’s clear he’s proud of the framework and what it means for the Māori community, who make up a big part of Totara Hospice’s demographic.
I ask Jap if his time as a palliative care doctor has changed his perception of his own mortality. “In my work, I see lost opportunities all the time. People haven’t had the chance to live their life.” Jap remembers one patient in particular because his story was so sad. “He’d worked his butt off for many years. He came to New Zealand because he’d seen Lord of the Rings and said, ‘oh what a lovely place, that’s what I want to come here for’. But he’d been working so hard he actually hadn’t gone anywhere apart from Auckland. His regret was that he hadn’t seen the country that he really wanted to see, which was why he’d come over in the first place.” That patient was only 40 years old when he died, and it’s stories like his that remind Jap to live without regrets.
There’s someone closer to him that he also takes inspiration from. “It all comes back to my Aunty Helen, who had a big influence on my life. She was always telling me when I was younger to enjoy life a bit, don’t save it up until later.” From the way Jap speaks about Helen – his eyes shining, effusive in his praise – you can tell she was someone who had a voracious love for life. She went on adventures all over the world, and when she was eventually diagnosed with heart disease and became very unwell, she’d done the things she’d wanted to do. Jap says he tries to give himself the “treats” of small trips away more often because of her legacy.
Being a palliative care physician means being around death with a frequency that might alarm the rest of us. It seems like the kind of job that requires a particular personality, and I ask Jap what that is. “You have to be emotionally strong enough to be able to be with people during a really stressful time. You do have to have a certain amount of emotional resilience. You need to have sorted out your own stuff as much as possible before you even consider it because if you’ve got open wounds yourself, you’re going to get triggered because you’re dealing with raw human emotion, raw human stressors.”
Jap removes his ID badge and his stethoscope and puts them away before he goes home each day, and it’s how he signals to his body that his work is done. He says he has very clear demarcation lines about work and his personal life, and that’s how he avoids taking his work with him when he leaves.
“Most of the time it works. But sometimes there are cases that get to you a bit more, because we’re humans, we have emotional feelings and we do connect with the people that we work with. If we can’t connect, we won’t be able to serve them as well.”
Jap also meditates and recently got into the Japanese art of forest bathing. He looks a touch embarrassed when he explains it to me. “Executives that are highly stressed and strung out get sent to go on walks in the forest. It’s like a meditative process, but you also hear the sights and smell the smells. Pine trees, for example, give off little things called terpenes which have a relaxing effect on human beings, and they can drop your blood pressure. So that’s the sort of thing I go and do. Just to the local parks and that sort of thing.”

Part of Jap’s self-care routine is debriefing with a professional supervisor every month. He also cultivates a deadpan sense of humour and has amassed a collection of over 40 cartoon ties, which he wears as a way to connect with patients. “I kind of wear them as a badge,” he says, flapping the end of his tie like a flag. “It’s like, ‘hey, you can talk to me’! I think that’s my favourite thing about being a doctor, is that I can still laugh with my patients, ‘cause let’s face it – there’s a lot to cry about.”
Around Totara Hospice, Jap is famous not only for his ties, but for his dad jokes, and recently got put in “prison” for them on the clinic’s Facebook page. It took $500 in donations to secure his release. He laughs when he tells me he has a Winnie the Pooh tie. “My standard dad joke for that is, ‘I’m the only doctor you’ll see who doesn’t mind having a bit of Pooh on his tie’.”
The father of two young children, Jap says death has been part of his kids’ upbringing from an early age. “When they were crawling toddlers and I was working weekends, I’d bring the kids in. Right from year dot, they know what I do for a job. They understand that death is part of life. They’re a bit more open to the concept of death than most kids would be I’d say.” There have been several deaths in Jap’s family in recent years, which has allowed the conversations around mortality to continue, but it was the death of his own mother in January this year that challenged him.
It was a time when Japs’ work had to come home with him as he supported his father through his mother’s decline, preparing him for what was coming. He had to wear the hat of both a child losing a parent and a palliative care doctor watching the end of a life. There’s sadness in him as he shares that he wasn’t with his mother when she died. For someone so often present at the deaths of strangers, it must’ve been difficult to cope with.
“Lets just say I’d been preparing myself, but even with my years of experience, it was quite a shock that she’d passed when I wasn’t there.”
It’s obvious from the way he talks – soft and slow, like he’s working it out – that he was grateful for the opportunity to share the wisdom gained through his work, but it also strikes me that his expertise couldn’t prevent him from the grief that death brings. He gives me a little smile and pushes his glasses back up his nose.
It’s one of the last things Jap says to me that stays with me most. We’re talking about his death and how he would like to go out (some kind of video production at his funeral, or a comic book, or something else unexpected) and he’s so easy and good-humoured about it. To me, it’s bizarre to be joking about our funerals, but Jap is matter-of-fact about it. “No one gets out of this life alive,” he says, checking his name badge is on straight. He thinks we’d do well to start talking about our own mortality and making plans for our inevitable deaths.
“We’re kidding ourselves if we think that we can control nature because that’s what we’re trying to do with medicine and healthcare. We’re trying to control the force of nature, and when you’re trying to control the force of something like a hurricane, you’re on a hiding to nothing.” He says it plainly, but with kindness, and then he shakes my hand and heads back to the ward.