
Woolworths has moved the buttons on its Eftpos machines, in what appears to be an effort to gaslight the nation and destroy the self-esteem of one Spinoff writer.
When I arrived at Woolworths this afternoon, I was excited to see a bewildered old man struggling to pay for his groceries. His pain was my gain. I’d been sent to the supermarket to check out a hot news tip from The Spinoff founder Duncan Greive, who’d urged his beleaguered website workers to investigate “chaos at the tills” caused by an alleged layout change to the Eftpos machines.
Though a single confused man is more depressing than chaotic, it was a promising start. I resolved to check out the checkouts myself for further information. After scanning a small bag of baby spinach we needed for dinner, I stuck my debit card in the Eftpos machine, extended my paying finger, and immediately fell back into my old habit of mentally cursing Duncan Greive.
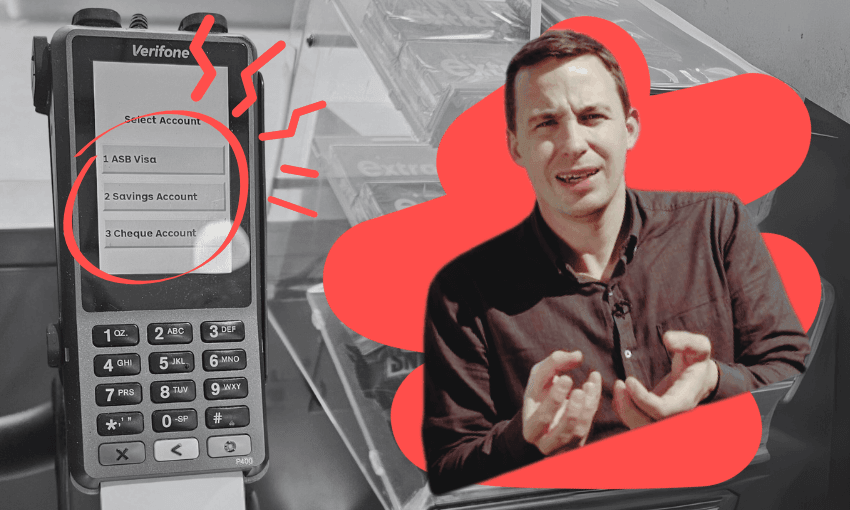
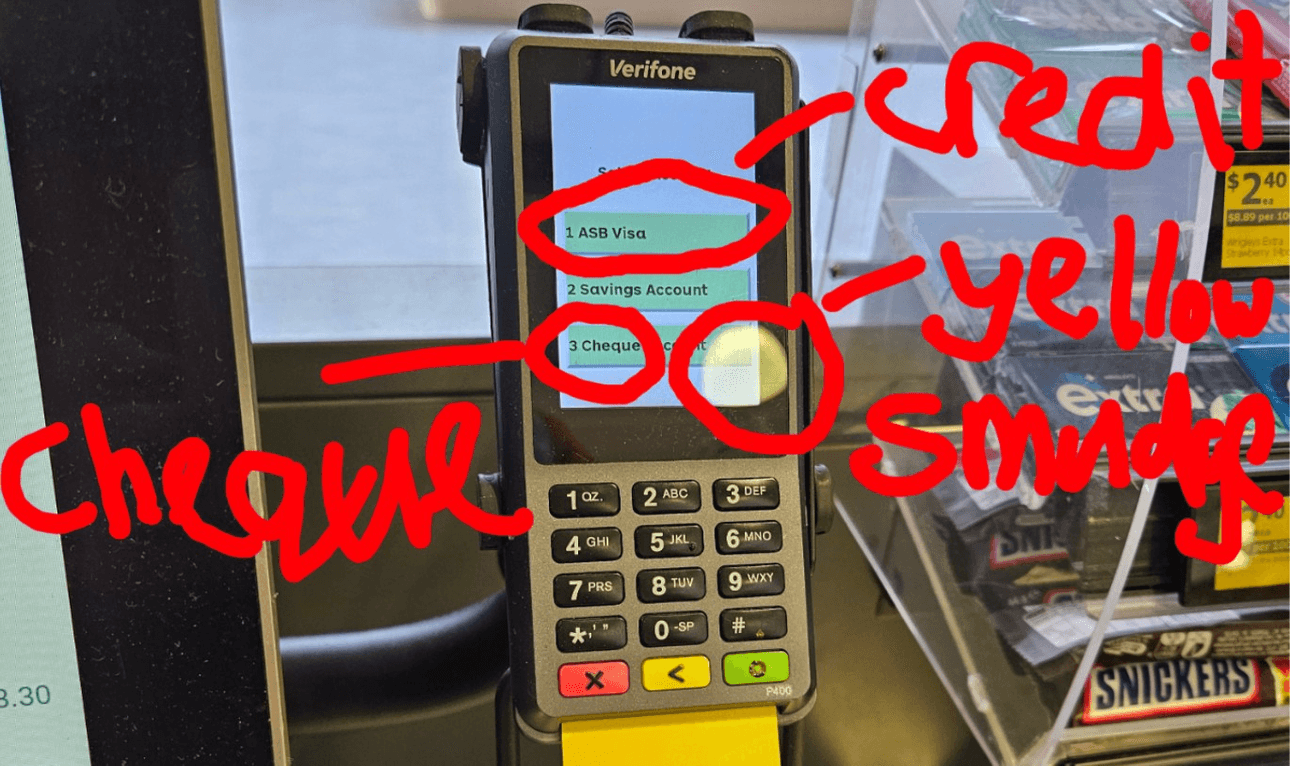
As I saw it, the founder of The Spinoff had wasted my time and probably money, because let’s be honest we could’ve done without the baby spinach. Though the Eftpos machine looked a bit different, it seemed the buttons were all in the same place. There was a word beginning with c next to the 3. 1 said ASB, which is the name of my bank, so that must be my cheque account.
If none of this makes sense, it’s because it’s the thought process of an idiot. Somehow, despite being almost uniquely blessed with foreknowledge of possible changes to Woolworths’ payment system, I’d still been caught out and pressed the wrong button.
The reality is Woolworths has changed its Eftpos layout. The 1 button, which used to summon your cheque account, is now the number to press to pay by credit card. Contrary to Greive’s misleading and probably defamatory assertions, 2 still links to your savings. But 3 is now the home of cheque.
When a checkout operator mercifully came to my assistance, I asked whether the switch had been causing chaos. She screwed up her face, then carried out a controlled demolition of my remaining self-esteem. “No, because most people sort of just work it out,” she replied.
This interaction would later inform my questions to Woolworths’ media team. “Have you had any reports from customers about confusion over the new Eftpos machine layout?” I led off. “Why have these changes been made?” These were journalistic fig leaves covering the real reason for my email, question 3: “Is the author of this piece for The Spinoff an idiot for somehow screwing this up despite knowing in advance the Eftpos layout may have changed?”
“What’s your deadline here?” replied the media team.
This was followed by a call from a Woolworths spokesperson explaining the relevant executives weren’t available to sign off a media statement by my deadline, which was within two hours. “So Woolworths’ official position right now is that I am an idiot?” I asked. “I couldn’t possibly comment,” said the media team member. “There’s a lack of appropriate data.”
All of a sudden, I was back at the entrance to Woolworths, looking at the checkouts. There was that confused old codger struggling to pay for his veges. But I looked closer. The old man was me, tapping furiously at an unresponsive terminal, trying to navigate a world I no longer understood. If you want to avoid the same fate, press 1 for credit and 3 for cheque.
Update, 11.45am, June 25: A Woolworths spokesperson says the Eftpos machine layout change was a mistake. It will soon be fixed and they “sincerely apologise”. The spokesperson failed to address questions about Hayden Donnell’s mental acuity.
The statement in full:
After finding a small glitch in the EFTPOS process we applied a fix. Unfortunately that changed the order that accounts appear here in New Zealand, leading to some customers having their cards declined because they pressed the ‘wrong’ number. We are reverting to the way accounts previously appeared and we sincerely apologise to any customers who have been affected. The change will take place as soon as possible and we suggest customers take a moment to check they are selecting the right option.